
If you're a smoker, read this article carefully. Even you're a non-smoker but one of your family members is a smoker, you should read it too.

There are about 1.2 to 1.3 billion people worldwide (about 17% out of the world's population) who fall prey to smoking, which brings on serious health problems. And Gary is a prime example.
Gary really enjoyed his youth, when he spent most of his time knocking about with friends. It was also the time that he started smoking.
"If I were able to choose, I'd have lived differently," reflected the Korean man now in his 60s. "I had smoked more than I should. Sometimes I was up to 30 sticks a day."
Years of heavy smoking have taken a toll on Gary's health. He started coughing and having difficulty breathing. His cough, sometimes non-stop, once embarrassed him at work. He had struggled with the symptoms and had to go to hospital several times over the past few years due to breathlessness.
"I'd tried all the bronchodilators I could find to ease my cough and help me breathe. But they didn't help much," he said.
Last year, his condition deteriorated and he was taken by ambulance to a hospital.
"It was like somebody put a plastic bag on my face. I nearly suffocated to death," Gary recalled.
It was touch-and-go whether the ambulance could rush to the hospital in time and the doctor would get there and save his life. His doctor told him that he had Chronic Obstructive Pulmonary Disease (COPD) and it had exacerbated. And the extent of chronic inflammation in his lungs and the narrowing of the airways made it hard for Gary's condition to stabilise. To reduce the risk of future COPD attacks, he has been treated with medication. Importantly, he changed his lifestyle.
After his first COPD experience, he found it sometimes difficult to make the slightest movement. Even eating became a real struggle for him. He was heavily dependent on his wife, his care giver, for everyday activities.
Despite his condition, Gary enjoys a happy life. He quit smoking. He is able to have light walks with his wife in a park and to have a good time with his grandson, Jack, who wants to be a pilot.
"My grandson is such a good boy and so smart too. It's so rewarding to watch him grow up," he said, beaming.
"I don't feel as fit as I used to but I'm happy that I can live again. I will do whatever it takes to avoid future COPD lung attacks."
Despite being a long-term lung disease that is hard on patients' physical and emotional well-being, COPD is often disregarded and under-diagnosed. The condition often coexists with other diseases including cardiovascular disease, lung cancer, serious infections, metabolic syndrome and diabetes, all of which can have a significant affect on prognosis. It's a lethal disease and claimed about three million lives in 2005.
The World Health Organisation (WHO) estimates that 65 million people worldwide have moderate to severe COPD. The disease is now the fifth leading cause of death worldwide and the WHO predicts it will become the third cause of death by 2030.
According to Prof Sumalee Kiatboonsri from the Division of Pulmonary diseases, Department of Medicine, Ramathibodi Hospital, COPD is a progressive lung disease that involves chronic bronchitis and emphysema.
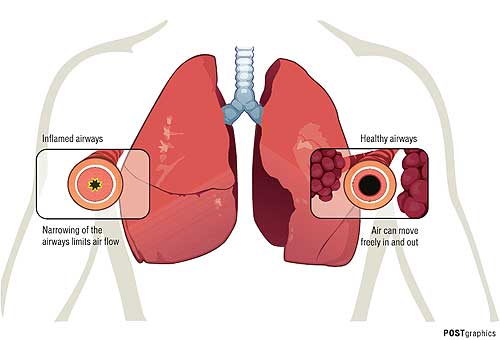
COPD develops slowly but gets worse over time. It distorts patients' airways, making them inflamed and partly blocked with mucus. The condition also damages the tiny air sacs at the tips of patients' airways.
"When a patient with COPD is exposed to noxious stimuli, the inflammation of the bronchioles develops and causes smooth muscles to contract and then obstruct airflow," said Dr Sumalee, who is also president of the Thoracic Society of Thailand.
One of the most frightening symptoms associated with COPD is lung attacks, or exacerbations, like Gary once experienced. Acute events marked by a worsening of a patient's respiratory symptoms, they may be caused by severe air pollutants, or viral or bacterial infection.
During exacerbation, patients may require hospitalisation or develop a life-threatening condition.
"An exacerbation makes an already bad situation worse. Frequent COPD flare-ups may cause a more rapid decline in lung function," said Assoc Prof Watchara Boonsawat from the Department of Medicine, Faculty of Medicine at Khon Kaen University.
Although COPD is mostly caused by tobacco smoking, non-smokers may also be affected when exposed to air pollution and occupational dusts and chemicals. It has been noted that indoor air pollution may also play an important role in the development and progression of COPD among people in developing countries.
"Chinese women, for instance, who live in rural areas and use biomass fuel for cooking and heating in poorly ventilated dwellings may have a high risk of COPD development when the exposure of the burning of biomass fuels are intense and prolonged enough," Dr Watchara said.
How symptoms progress varies, but patients may develop a mild cough that produces sputum around the age of 40. The cough and sputum production typically becomes persistent, and shortness of breath occurs with physical exertion.
"As COPD symptoms are not specific, suspected patients may be asked to have spirometry diagnosis, a simple lung function test which along with the presence of such symptoms helps give an accurate diagnosis," Dr Sumalee said. "By doing the test, patients force the air out of the chest as hard and fast as they can until their lungs are completely empty. The test measures how much air patients can move out of their lungs and the amount of time they take to do so."
The doctor said the test also helped gauge the severity of disease and could guide treatment.
"Giving a lung test for a patient is not an easy task," Dr Sumalee said. "Each patient has different levels of ability with spirometry. I can finish working with an able patient who receives the test within 10 minutes. But it can take a much longer time, sometimes half a day, for a patient who is not comfortable with the test."
Tools for COPD diagnosis are available at the country's leading hospitals, Dr Watchara added, but there was a shortage of skilled healthcare professionals who could administer the test. He also noted that most patients were not aware of the lung function test.
"When having chronic cough and difficulty breathing, most of them ask for a chest X-ray," said Dr Watchara, who is chairman of the Easy Asthma and COPD Clinic Network and president of The Thai Asthma Council and Association. "The chest X-ray in mild COPD cases is usually normal. When results show that there is nothing unusual during the physical examination, they continue smoking."
If patients with COPD don't catch the condition, they may have more symptoms over time and their lungs may become more damaged, making it more difficult to treat, he said.
Dr Sumalee said: "If you smoke, quit as soon as possible. It's never too late to quit smoking even when you're diagnosed with COPD.
Stopping smoking at any point in the disease process gives some benefit. In fact, it can improve many other health conditions apart from COPD."
Currently there is no cure for COPD but the disease is treatable. Treatment is aimed at relieving and reducing symptoms as well as decreasing the risk of exacerbation in the future.
"About 90% of COPD medication comes in inhaled form. Patients have to learn to use it correctly in order to benefit from it," Dr Sumalee said.
"Pulmonary rehabilitation and improving exercise tolerance are important parts of COPD treatment. They can help enhance quality of life."
Many patients and even some doctors have felt desperate with COPD over the years. But Dr Watchara said the concept of COPD treatment had changed over the past decade, thanks to medical advances and research studies.
"COPD is a common preventable and treatable condition," Dr Watchara said. "We've learned more about inflammation mechanisms related to it. We now focus not only on the use of bronchodilators, but also the treatment of inflammation cells to manage with the condition."
Landmark study in Asia
Early this year, the "Epidemiology and Impact of COPD in Asia" survey (EPIC Asia Survey), a large-scale community-based study, was conducted by Takeda. This was the first study of its kind in Asia.
"There was a gap in the knowledge about COPD," Prof Sam Lim, chairman of the EPIC Asia Survey committee, said at a press conference in Seoul last month. "When you ask Asian physicians, they may say, 'I don't really know why my patients have a lot of coughing'. And I don't really know that our patients have as many exacerbations as Western populations. We need data on Asian patients to be sure that Asian patients behave in similar ways to Western ones. And the EPIC Asia survey will help fill the gap in the knowledge about COPD in Asia."
About 112,330 households in Thailand, China, Hong Kong, Indonesia, Malaysia, the Philippines, Singapore, Taiwan and Vietnam were screened for COPD.
Of these households, there were 1,841 respondents, aged 40 or older, who were diagnosed with COPD or have COPD symptoms, including chronic obstructive airway disease (COAD), chronic obstructive lung disease (COLD), chronic bronchitis or emphysema and who meet the symptomatic definition of chronic bronchitis.
The key findings show that the prevalence of the disease among patients aged over 40 was an estimated 6% in Asia.
About 41% of them were still under-diagnosed and 19% of them fell into the severe phenotype category, experiencing coughing and sputum with frequent COPD lung attacks.
About 37% of respondents were unable to work because of their condition. Sixty-one percent of respondents who are able to hold a job missed days at work due to their condition. And the average days of missed work were 13 in the last 12 months. About 46% of subjects had suffered a flare-up in the past 12 months.
And the episode of worsening symptoms lasted about 13 days on average.
COPD in Thailand
About 214 Thai respondents participated in the survey. Findings revealed that the prevalence of COPD in Thailand was an estimated 5%.
And two-thirds of patients with COPD symptoms remain undiagnosed. About 61% of Thai participants surveyed had seen a doctor or other healthcare provider because of respiratory exacerbations or worsening symptoms.
Six out of 10 worried about having COPD lung attacks when they are away from home, while more than three out of 10 were not employed full time due to COPD.
Half of those employed full-time missed work in the past year due to their condition.
Asthma or COPD?
COPD is often confused with asthma, but the two are very different.
Asthma usually starts early in life, usually during childhood, while the onset of COPD is in mid-life, often afflicting people aged over 40.
"There are two useful distinguishing features," said Prof Peter Calverley, from Pulmonary and Rehabilitation Medicine at the University of Liverpool.
Firstly, when asthmatics use an inhaler, the symptoms are often relieved. And symptoms and signs pass quickly. However, the problem with a COPD attack is that it comes on slowly but lasts much longer and has a greater impact on patients. As a result, the timing of systematic attacks and recovery is different. There is also a difference in sleep patterns.
COPD patients sleep badly, but they usually don't wake up with attacks of wheezing and tightness in the chest.
"Another thing, people who start with asthma and smoke often end up with COPD," said Dr Calverley, adding that people with asthma when they were young may grow out of it, but if smokers don't quit, they may well develop COPD instead.
Prof Dr Sumalee Kiatboonsri, an expert at the Department of Medicine, Ramathibodi Hospital, added that during spirometry diagnosis, the airflow obstruction in asthmatics is generally reversible following medication.
That is in contrast with the airflow obstruction of COPD which is not fully reversible.
